

The Trauma Myth
The power of the trauma myth is undeniable. It validates mental suffering, provides meaning, and offers the hope of salvation. Yet behavioral genetics will tear this myth asunder.

Written by Ben Winegard and Bo Winegard.
Bessel van der Kolk, an affable octogenarian, has emerged as an unlikely spiritual guru and minor celebrity. His book, The Body Keeps the Score, has spent 240 weeks on the New York Times best seller list and sold more than 2 million copies worldwide. It is currently number 7 on Amazon Charts, a list of the week’s best sellers. Over 66,000 readers have reviewed the book on Amazon. Most reviews are effusive, calling the book “ground breaking,” “life changing,” and “transformative.” The book itself is a compelling blend of anecdote, myth, and self-help bromides generously seasoned with scientific terminology (epigenetics, hypothalamus, amygdala, anterior cingulate). van der Kolk’s message: Trauma is the root of much of our suffering. Often we evade this reality–our minds warp, distort, and repress. Our bodies and brains, however, produce a steady potpourri of symptoms: panic attacks, depressive episodes, bipolar illness, borderline personality, chronic fatigue, fibromyalgia. Fortunately, this suffering is not inevitable. By acknowledging our trauma we can be healed and made whole.
The power of the trauma myth is undeniable. It validates mental suffering, provides meaning, and offers the hope of salvation. Humans suffer not because they are fallen or because of difficult-to-understand impersonal forces such as genes, but because they have been violated and victimized.
However, many of the empirical claims in The Body Keeps the Score do not withstand scientific scrutiny. Unlike other myths, the trauma myth claims to be grounded in the latest findings from epidemiology, neuroscience, endocrinology, genetics, and biology. And it makes evidence-based claims about effective modalities of treatment. To the extent these claims are hyperbolic or false, they have potentially profound and deleterious consequences. For one example, van der Kolk confidently asserts that “hundreds of scientific publications spanning well over a century” document the reality of repressed memories. Yet, the consensus of memory experts is skeptical and the recovered memory movement has led to myriad false accusations of child sexual abuse.
In this article, we will focus on the claim that borderline Personality Disorder (BPD) is (mostly) caused by childhood trauma, especially childhood sexual abuse. We focus on BPD for a few reasons. First, of all common mental disorders, with the exception of PTSD, Borderline Personality Disorder is most commonly associated with childhood trauma. As one piece of evidence, a Google search of “Trauma and borderline personality disorder” brings up over 9 million results. Indeed, a few prominent scholars, including Bessel van der Kolk, have argued that BPD should be considered a trauma-spectrum disorder.
Second, there is a move toward destigmatizing BPD premised on the idea that those who suffer should be viewed as victims rather than “perpetrators of their own misfortune.” This is misguided. The etiology of a particular disorder should not dictate whether or not it is stigmatized by society. It is unclear why BPD should be less stigmatized if it is caused by trauma than if it is caused by genetics and random environmental factors.
One can take a compassionate approach to the suffering caused by borderline personality disorder (both to the patients and their loved ones) while being scientifically rigorous and honest about the underlying etiology.
And, third, many high quality genetically informed studies of BPD are available which allow us to control for confounding variables and disentangle the role of genetics and the environment. And this allows us to examine one hypothesis of the trauma-myth with sharp focus. If the trauma theory of BPD does not hold up, then this at least casts doubt on other claims of the trauma myth.
What is borderline personality disorder?
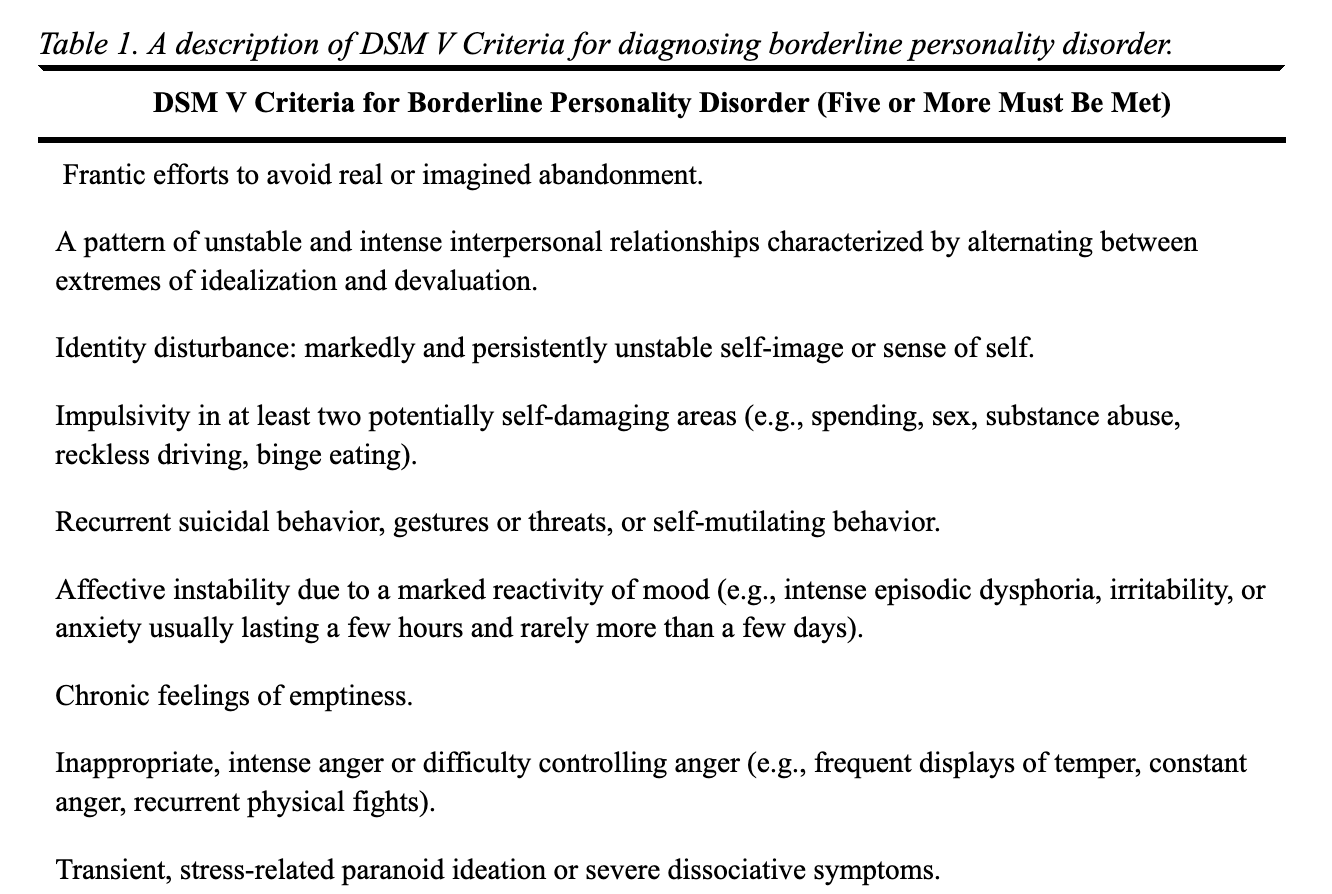
The term "borderline personality disorder" (alternatively, BPD) was initially coined by Adolf Stern in 1938 to describe patients who did not fit into the categories of psychosis or neurosis. In 1975, John Gunderson and Margaret Singer published a review article outlining the defining characteristics of BPD, which include intense interpersonal relationships and impulsivity. While the term itself is somewhat contentious, and the presentation of BPD varies among individuals, there is a general consensus regarding certain core features (refer to Table 1 below for DSM V criteria).
Typically, individuals with borderline personality disorder have a history of turbulent and unstable interpersonal and romantic relationships. They often oscillate between idealizing and devaluing others; experience identity instability with rapidly shifting norms, values, and goals; exhibit disinhibition and impulsivity in multiple domains; engage in self-mutilation and suicidal behavior; display pronounced mood reactivity and emotional sensitivity, and make frantic efforts to avoid real or perceived abandonment by loved ones.
Estimates of the lifetime prevalence of borderline personality disorder vary considerably depending on the sample and method of assessment. A comprehensive review of studies reported a lifetime prevalence of 9.7% among college students, while a review of point prevalence in community settings estimated that 1% of individuals had Borderline Personality Disorder.
Borderline Personality also exhibits high levels of comorbidity. For instance, a study analyzing data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), which included 34,481 participants, revealed that 83% of individuals with BPD had experienced a lifetime mood disorder or episode, 85% had a lifetime anxiety disorder, and 78% had a lifetime substance use disorder. A notable Swedish register study, involving over 11,000 clinically diagnosed BPD individuals, found that 95.7% had received at least one other psychiatric diagnosis, with anxiety disorders (75.7%), affective disorders (76%), and substance use disorders (48.6%) being the most prevalent co-occurring conditions.
BPD is associated with high morbidity and mortality and is overrepresented in inpatient settings. Perhaps most alarming is the substantial increase in the risk of suicide attempts and completed suicides among individuals with BPD. It is estimated that approximately 75% of diagnosed individuals will make at least one suicide attempt, with 2-5% completing suicide within 5-14 years after diagnosis, and 8-10% completing suicide within 15-27 years after diagnosis.
General Hypotheses about BPD and Childhood Trauma
There are three broad hypotheses that can account for an association between borderline personality disorder and childhood trauma (see Figure 1 below).
Environmentalist Hypothesis (The Simple Trauma Myth): There is a causal relationship between childhood trauma and the development of borderline personality disorder, with the environment playing a determinative role. The environmentalist hypothesis posits that any child or adolescent who experiences trauma has the potential to develop Borderline symptoms, and in severe instances, progress to clinical borderline personality disorder. Moreover, this hypothesis suggests a dose-dependent response, meaning that trauma severity positively correlates with severity of Borderline symptoms. Unlike the other hypotheses, genetics are not considered a causal factor in BPD development, resulting in low to zero heritability, while the influence of shared environmental factors is predicted to be moderate to large.
Biosocial Hypothesis (The Sophisticated Trauma Myth): The relationship between BPD and childhood trauma is causal, but only people with a certain diathesis develop Borderline symptoms after experiencing trauma (gene-environment interaction = GxE). In diathesis-stress models of borderline personality disorder, the heritability can range from moderate to high while shared and/or unshared environmental effects are expected to contribute to variation in Borderline symptoms.
Genetic Confounding Hypothesis: The observed relationship between borderline personality disorder and trauma is spurious and is caused by a correlation between genetics and the environment (rGE). That is, the genes that are associated with BPD are also associated with environments characterized by higher rates of traumatic experiences. For instance, parents who possess traits such as low impulse control and high emotional reactivity may pass on genes related to those traits to their offspring. Furthermore, these same parents are more likely to create chaotic home environments and physically and emotionally abuse their children. From this viewpoint, the trauma experienced is not causal; instead, it is the genes transmitted from parents to offspring that contribute to the development of BPD.

rGE = Gene environment correlation. In the figure, the path from trauma to BPD runs through genes and is not causal. GxE = gene environment interaction. Trauma is causally linked to BPD, but the effect is moderated by an individual’s genes.
Theories Linking Trauma to Borderline Personality Disorder
Researchers have forwarded myriad theories from the environmentalist and biosocial perspectives to explain why childhood trauma would be causally linked to borderline personality disorder. The theories are not not necessarily mutually exclusive, but possess differences of emphasis.
Judith Lewis Herman introduced the concept of complex PTSD to explain a set of symptoms stemming from chronic exposure to extreme stress, particularly in situations where an individual is under the control of another person, such as in prison camps or abusive families. Herman observed that survivors in these circumstances exhibited a symptom profile that was more intricate, diffuse, and difficult to treat compared to simple PTSD. According to Herman, borderline personality disorder can be viewed as a trauma-spectrum disorder, in which the core symptoms of Borderline are adaptive or maladaptive responses to an environment characterized by chronic abuse and control. For instance, dissociation may serve as a coping mechanism for Borderline patients to navigate an overwhelmingly horrific reality, while depression may arise from a profound loss of faith and hope. Additionally, somatic symptoms like headaches and gastrointestinal disturbances may emerge because of prolonged hypervigilance and the resulting stress on the individual's body.
Bessel van der Kolk and his colleagues proposed that experiencing prolonged and severe trauma, particularly during childhood, can result in difficulties in adaptive emotion regulation, a fragmented sense of self, and developmental stagnation. They suggested that the symptoms of borderline personality disorder are attempts by individuals to self-soothe using coping mechanisms developed during traumatic experiences. For instance, dissociation serves as a means to cope with overwhelming stress by constricting consciousness and detaching from both physical and psychological distress. Additionally, the phenomenon of splitting, which involves oscillating between extreme idealization and devaluation of others, reflects patterns of interaction carried over from childhood and a lack of integrated personality.
Laura Kaehler and Jennifer Freyd argued for a more specific link between betrayal trauma and Borderline Personality traits. Betrayal trauma occurs when caregivers or parents, who should provide support and safety, become the source of trauma. Since a child's attachment to these individuals is crucial for their survival, they often feel compelled to maintain the relationship even in the face of severe abuse. To cope with betrayal trauma, individuals may employ strategies such as dissociation, amnesia, and repression to keep the threatening information from entering their full conscious awareness. Therefore, individuals suffering from betrayal trauma are predicted to have attachment issues (lack of trust) and cognitive dissociation, which are symptoms typical of BPD.
Marsha Linehan proposed the influential biosocial theory, which has emerged as the most prominent theory linking childhood trauma and Borderline Personality Disorder. According to Linehan, a combination of specific biological vulnerabilities and environmental influences contribute to the manifestation of Borderline symptoms (GxE). The central biological vulnerability is emotional dysregulation, which results in heightened emotional sensitivity, an inability to effectively regulate intense emotional responses, and a slower return to emotional equilibrium. When vulnerable individuals are raised in environments that discourage or respond erratically and inappropriately to the expression of private experiences and emotions ("invalidating environment"), they fail to learn the necessary tools to regulate their emotional responses. Consequently, these individuals often experience emotional instability, exhibiting oscillations between emotional extremes and displaying high levels of emotional lability–all hallmarks of BPD.
While the above theories focus on proximate psychological–and, to a lesser degree, physiological–mechanisms that lead from childhood trauma to Borderline Personality Disorder, some recent theories focus on ultimate or evolutionary explanations. From an evolutionary perspective, certain Borderline symptoms may be viewed as an adaptive response to high levels of childhood adversity. Specifically, adversity in childhood may be interpreted as a marker of high extrinsic mortality rates and low paternal investment and lead to a shift from long-term somatic maintenance toward immediate reproductive goals. From this perspective, the elevated aggressiveness, insecure attachments, impulsivity, and sexual promiscuity seen in Borderline patients can be viewed as manifestations of a shift toward a fast life history strategy.
Supporting the life history theory, evidence from a nationally representative survey in the United States, found that Borderline traits were negatively associated with age at first intercourse and positively associated with number of children and number of marriages.
The first three of these theories are species of the trauma myth and mostly environmentalist in orientation, while Linehan’s biosocial theory and the evolutionary-based life history theories represent more sophisticated versions of the trauma myth and are consistent with the biosocial hypothesis. The environmentalist position can be tested through a combination of the observational studies and classical behavior genetics. A more rigorous method of causal inference is necessary to distinguish between the biosocial hypotheses and the genetic confounding hypothesis.
Evidence Linking Trauma to Borderline Personality Disorder
Early causal studies of borderline personality disorder were psychodynamic in orientation and focused on parental separation or loss and disturbed parenting. Beginning in the late 1980s, researchers began to explore the link between a range of childhood traumas (including physical and sexual abuse) and the development of borderline personality disorder. Generally, researchers used retrospective case-control methods, comparing patients with diagnosed borderline personality disorder to clinical non-Borderline controls.
For example, Herman, Perry, & van der Kolk (1989) compared 23 Borderline patients with 21 clinical controls. They found that 81% of BPD patients suffered trauma while only 52% of controls did. BPD patients experienced sexual abuse at more than twice the rate as the non-BPD group (67% to 26%). Similarly, Westen and colleagues (1990) found that BPD patients suffered more physical abuse, sexual abuse, and neglect than clinical controls. These early case-control studies are summarized in Table 2. The results of the six studies are quite consistent. In each of them, borderline personality disorder was associated with higher levels of overall childhood trauma, physical abuse, and sexual abuse than clinical controls.

References: Links, Herman, Zanarini, Ogata, Westen, Goldman
Although consistency of association is an important criterion for inferring causality, it is not sufficient. Further, case-control studies suffer from many potential biases (e.g., recall bias), are incapable of ruling out confounding variables, and, thus, are generally not considered high-quality evidence. However, more recent prospective cohort studies have found a similar association between childhood trauma and subsequent development of Borderline Personality Disorder, as have epidemiological studies based upon representative samples. The association between childhood trauma and BPD has been documented in numerous countries (e.g., Turkey, Germany, Canada, The Netherlands, Brazil, and South Korea).
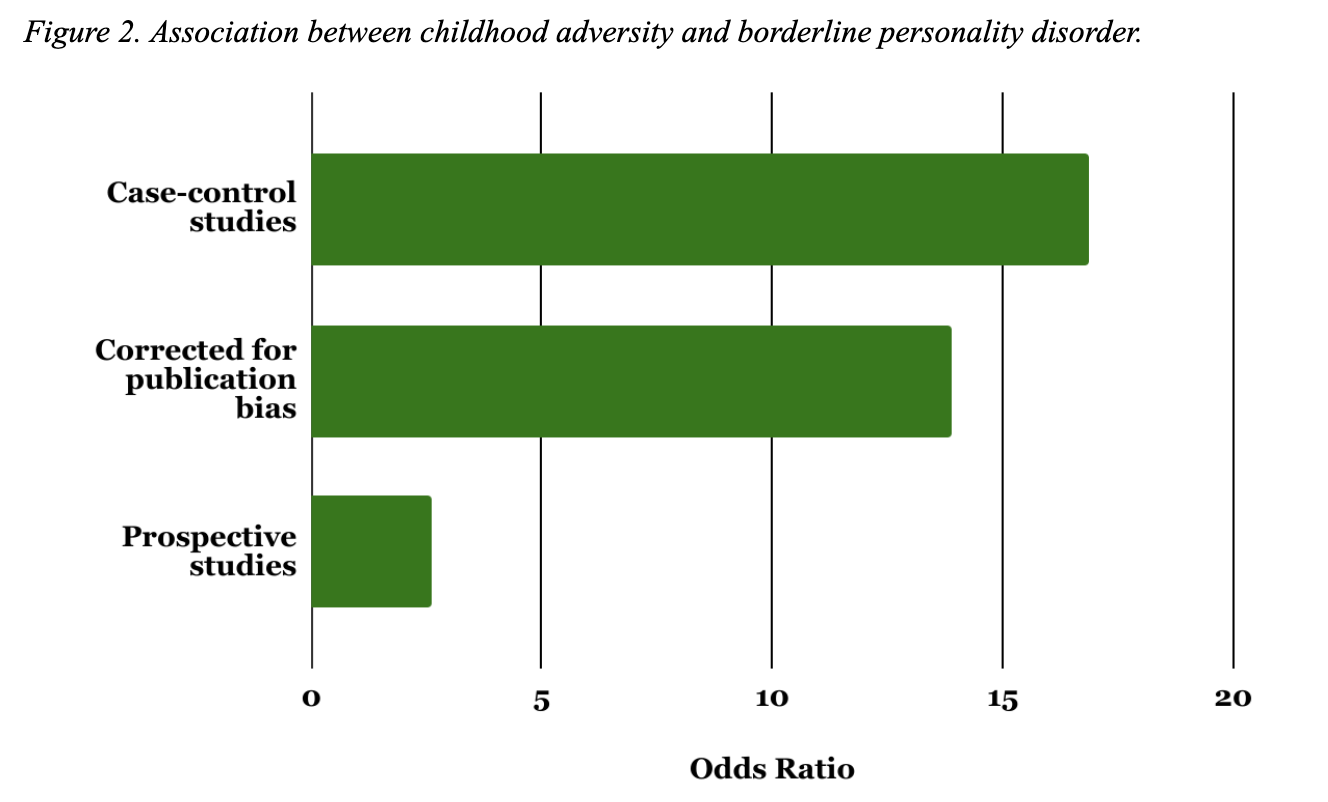
The most comprehensive and up-to-date review of observational studies, a 2020 meta-analysis including 97 studies, found 71% of those with borderline personality disorder reported at least one adverse childhood experience, with 48.9% reporting physical neglect, 42.5% reporting emotional abuse, 36.4% reporting physical abuse, and 32.1% reporting sexual abuse. In case studies comparing BPD individuals to non-clinical controls, the odds ratio was 16.86 for any adversity, 9.18 for physical abuse, and 6.76 for sexual abuse. When compared to clinical controls, the odds ratios ranged between 2 and 4.
Another criteria for causal inference is dose dependency. In early case-control studies of smoking and lung cancer, for example, a dose dependent relationship between number of cigarettes smoked per day and probability of lung cancer was discovered. This was an important factor in concluding the relationship was causal.
Most studies of childhood trauma or abuse and BPD have found that more severe trauma is in fact related to worse symptoms and a poorer prognosis. A few representative examples: Zanarini and colleagues (2002) found that severity of trauma was linked to severity of symptoms in affect, cognition, impulsivity, and interpersonal relationships among 290 Borderline inpatients. Watson and colleagues (2006) found a significant correlation between emotional abuse, physical abuse, emotional neglect and levels of dissociative symptoms in 139 borderline patients. In a population-based community sample, Hengartner and colleagues (2013) found a dose-response relationship between a total childhood adversity scale score and BPD. They also noted that reported childhood adversity explained 27.8% of the variance in borderline symptoms. Lastly, Turniansky and colleagues (2019) investigated the inpatient records of BPD patients with prolonged sexual abuse and found they had more hospitalizations, suicide attempts, and higher rates of alcohol use than non-exposed BPD patients.
In an systematic review of the topic, Jeffrey Ball and Pall Links argue that the relationship between childhood trauma and BPD fulfills most of Bradford Hill’s criteria of causality including a strong association, biological plausibility, consistency, dose-dependency, and temporality. They conclude:
It seems likely that as we pursue the study of BPD etiology, an integrated, multifactorial model ultimately will be adopted. We do not dispute that the etiology of BPD is likely multifactorial. However, we would argue that based on the evidence, particularly Hill’s criteria [of causality], childhood trauma plays a role in this model as an etiologic factor. [Emphasis added]
Getting at Causality
The evidence presented above seems strong and is backed by some of the most prominent experts in borderline personality disorder. However, there are severe limitations to causal inference from observational research. No matter how consistent the association between childhood trauma and BPD symptoms, scholars cannot control for all of the potential confounding variables in these research designs. As one example, the hypothesis of genetic confounding is impossible to test in absence of genetically informed research designs. Further, it is possible that the literature is marred by publication bias and that this may inflate the size of the association between childhood trauma and Borderline traits. Finally, it is possible that the effect size is inflated by reverse causality if individuals with borderline personality disorder overreport (for any reason) childhood trauma in retrospective studies and surveys.
Publication Bias, Methodological Quality, and Reverse Causality
Porter and colleagues (2020) formally checked for publication bias in their comprehensive meta-analysis. They found, overall, the odds ratio between childhood adversity and BPD dropped by almost 18% in case-control studies when corrected for publication bias (OR from 16.86 to 13.91) (See Figure 2 below). Further, the effect sizes were much smaller in epidemiological studies (2.56) and prospective cohort studies (2.59) than in case-control studies. Notably, the odds ratio for sexual abuse was substantially smaller (1.46) in the prospective cohort study than in case-control studies (5.96).
There are many possible explanations for finding smaller effects in prospective studies. It’s also important to note that there were only two studies based on representative samples and two prospective cohort studies (and only one that assessed childhood sexual abuse). One plausible explanation is that case-control studies select individuals with more severe symptoms of BPD who are often in inpatient treatment facilities. These individuals are likely to have more severe childhood trauma histories than individuals with more moderate BPD symptoms.
However, given that those with borderline personality disorder suffer from fraught interpersonal relationships and often end up devaluing family members and loved ones, it is also possible that such individuals are prone to reinterpret ambiguous childhood events and interactions as traumatic to form a meaningful narrative that helps rationalize their mental distress, chronic feelings of emptiness, loneliness, and relationship difficulties. In this scenario, dissonance reduction and post-hoc justification lead to over-reporting of trauma in retrospective studies.
Another possibility is that individuals with borderline personality disorder are at heightened risk to confabulate memories of childhood abuse and trauma that they believe they repressed. This may be especially likely in the case of individuals in therapy. A large, nationally representative survey found that of 1,082 individuals receiving therapy, 20.1 percent reported that their therapist discussed the possibility that they were abused as a child and repressed the memory. And 11.3% reported that they came to believe they were abused as a child when they previously had no such memory. Individuals with Borderline Personality Disorder utilize psychiatric services and individual therapy at a high rate, so if even a small percentage come to believe they were abused this could significantly distort retrospective assessments of childhood trauma.
Finally, it is likely the case that a small minority of BPD individuals fabricate histories of sexual, physical, and emotional abuse to gain sympathy and manipulate others.
Heritability and Discordant Twin Studies
After taking into account publication bias and methodological quality, we can conclude that the environment-only hypothesis is implausible. While it is not possible precisely to estimate the magnitude of association between childhood trauma and borderline personality disorder, it is almost certainly far lower than case-control studies indicate and lower than the observed association between smoking and lung cancer. Most individuals who are diagnosed with borderline personality disorder have not suffered from severe trauma as children and most individuals who suffer from severe childhood trauma do not develop Borderline Personality Disorder.
If borderline personality frequently develops in the absence of childhood trauma, other causal factors must be significant. Behavior genetic studies allow more direct causal tests about BPD and trauma. The environmentalist hypothesis predicts that genetic differences do not account for significant variance in borderline symptoms and further predicts that the shared environment will account for much of the variance. This is because childhood trauma is often shared within a household. In one study, for example, the shared environment accounted for 46% of the variance in self-reports of childhood abuse and 65% of self-reports of childhood sexual abuse. If childhood trauma makes siblings more alike on Borderline traits and is often shared within a household, this will show up as a shared environmental effect.
Over the last fifteen years, numerous behavioral genetic analyses have examined Borderline Personality disorder in multiple countries. A representative sample of these is summarized in Table 3 below. The results of these studies are surprisingly consistent: the heritability of borderline personality disorder is between 30% and 67% (Median = 42.2%) while the rest of the variance in Borderline traits is due to unshared environmental factors. The largest such study, which included 11,665 individuals with diagnosed Borderline Personality Disorder, estimated the heritability at 46% and concluded that shared familial environmental factors “are unlikely to contribute substantially to the etiological underpinnings of BPD.” Thus, BPD appears to operate similarly to thousands of human physical and psychological traits where twin resemblance and family aggregation is due solely to genetic variation.

References: Distel, Bornovalova, Torgerson, Reichborn-Kjennerud, Czajkowski, Skaug, Skoglund
Also of interest, the genetic factors that place a person at risk for developing borderline personality disorder are not specific to borderline pathology; instead they are shared across other personality disorders and psychopathologies including narcissistic personality disorder and obsessive-compulsive personality disorder. The few genome-wide association studies to date on BPD demonstrate that it shares a genetic liability with neuroticism, bipolar disorder, major depressive disorder, schizophrenia, and ADHD.
This effectively falsifies the environmentalist hypothesis. First, individuals in the same household do not become more alike on Borderline symptomatology because of shared trauma, including childhood sexual abuse, physical abuse, and emotional abuse. And second, it is clear from behavior genetic and genome-wide association studies that there is a substantial genetic liability to BPD and this risk is shared across a broad range of psychopathologies, which accounts for the observed phenotypic correlation between BPD and other disorders.
On the other hand, these findings are potentially consistent with the biosocial hypothesis in which a general biological vulnerability (e.g., negative emotionality or emotional dysregulation) interacts with environmental factors to produce Borderline symptoms. Classical twin and behavioral genetic studies are not able to distinguish between the genetic confounding and biosocial hypotheses of BPD pathogenesis. However, the discordant twin design controls for genetic confounding as well as the presence of GxE interactions and, thus, provides a “particularly stringent” test of causal effects.
Discordant twin studies investigate the association between an exposure and outcome of interest among unrelated individuals and compare the effects of this association to a set of discordant MZ and DZ twins. Researchers can then assess the strength of association between exposure and outcome in the overall sample and compare it to the effect observed within twin pairs discordant on the exposure. MZ twins reared together share a common environment and are genetically (almost) identical, while DZ twins reared together share a common environment and half of their segregating genes. Thus, the MZ within pair effect controls for both genetic and shared environmental factors and the DZ within pair effect controls for shared environment and partially for genetic factors.
In assessing the relationship between childhood trauma and Borderline symptoms, three general patterns might emerge: First, if the effect of trauma is purely causal, the association should be as strong in the discordant MZ and DZ twins as it is in the overall sample (i.e., controlling for genes and shared environment will not attenuate the effect). Second, if the relation is confounded by shared environmental factors, the MZ and DZ association will be similar and there will not be an association in the overall sample. Third, if the relation is due to genetic confounding, the effect will be found in the overall sample, will be attenuated among DZ twins (partial control for genetics) and will be absent in MZ twins (complete control for genetics). The biosocial hypothesis predicts there will be partial genetic confounding, but there will still be a significant relationship between childhood trauma and Borderline symptoms in discordant MZ twins whereas the genetic confounding hypothesis predicts this relationship will be non-significant.
To date, three studies have investigated childhood trauma and BPD with discordant twin designs. The first of these (2013) included 616 twin pairs (combined MZ and DZ) discordant on childhood trauma from the Norwegian National Medical Birth Registry. Overall, there was a significant association between childhood trauma and Borderline symptom criterion counts, consistent with the observational research reviewed above. This remained significant in the discordant twin sample, although it was reduced by over 50% compared to the full sample, which suggests significant familial confounding. Unfortunately, this study is limited by use of self-report data, a lack of variability in Borderline symptomatology, and the results of DZ and MZ discordant twins were pooled instead of analyzed separately. Overall, the results point toward at least partial genetic confounding but do not allow for strong causal inference.
A second study (2013), included 1382 twins from the Minnesota Twin Family study of which there were 197 MZ twin pairs and 137 DZ twin pairs discordant on childhood abuse. Consistent with association studies, they found an overall relation between childhood trauma and borderline personality disorder. The authors directly tested a diathesis-stress model by looking for an interaction between childhood abuse, internalizing, externalizing, and Borderline Personality traits. They found no evidence that childhood abuse had a greater effect in those high in internalizing or externalizing symptoms. Further, and consistent with genetic confounding, the relation between child abuse and Borderline traits was reduced in discordant DZ twin pairs and practically nonexistent in discordant MZ pairs. As with the first study, limitations included self-report and a small number of individuals meeting a clinical borderline personality disorder diagnosis.
The most recent study (2022) used semi-structured interviews, which possess greater validity, rather than self-report surveys to assess childhood trauma exposure. The overall sample consisted of 2,808 twin pairs from the Olso University Adolescent and Young Adult Twin Study. Of these, there were 158 MZ twin pairs and 325 DZ twin pairs discordant on any trauma. There was again an association between childhood trauma and BPD symptoms. However, this association was significantly attenuated in the discordant DZ twins and reduced to non-significance in the MZ twin pairs. Of the four trauma categories (emotional abuse, sexual abuse, physical abuse, and witnessing violence), only emotional abuse was significantly associated with Borderline symptoms in the discordant MZ twin pairs. But, the overall results of emotional abuse matched what would be expected from the genetic confounding hypothesis: The effect was largest in the overall sample and was twice as large in the discordant DZ pairs as the discordant MZ pairs.

Bars represent average differences in Borderline symptoms between individuals exposed to childhood trauma and individuals unexposed to childhood trauma.
All three of the discordant twin studies point toward significant, and perhaps complete, genetic confounding between Borderline symptoms and childhood trauma and two of the three rule out a significant GxE interaction. Instead, the link between childhood trauma and BPD is best explained by a correlation between genetics and the environment (rGE; See Figure 1). This suggests that the currently popular biosocial model of borderline personality disorder is likely false. The evidence, taken in toto, suggests a minimal to nonexistent causal role for childhood trauma in the development of borderline personality disorder. Rather than being “rooted” in trauma, BPD appears to be rooted in genetics, unpredictable life events, and stochastic developmental processes. Perhaps this is why no reliable causative environmental factor has been identified for borderline personality disorder. Instead, it might be time to embrace the gloomy prospect that, sans genetics, we will not identify any life events or environmental factors that help us understand why one individual develops Borderline Personality Disorder and another does not.
Conclusion
Over forty years of research has demonstrated a consistent association between childhood trauma and multiple mental disorders including borderline personality disorder, bipolar disorder, and major depressive disorder. A recent umbrella meta-analysis concluded that “psychological trauma is a transdiagnostic construct associated with nearly triple the risk of experiencing psychopathology.” According to the trauma myth, this association is causal and evidence of the vast suffering psychological trauma inflicts upon the human brain and body. Indeed, according to Bessel van der Kolk, the ontological status of mental disorders themselves should be called into question:
“How do we treat people who are coping with the fall-out of abuse, betrayal and abandonment when we are forced to diagnose them with depression, panic disorder, bipolar illness, or borderline personality, which do not really address what they are coping with?”
Trauma is the ultimate reality while specific physical and psychological symptoms are best viewed as emanations arising from the impact of trauma. To cure the person, we must address the deep-seated wounds caused by childhood traumas. How? One avenue is through talking, naming the evil, and processing the feelings and memories of the trauma. Others include taking antidepressant medications to dampen the “inappropriate” physiological alarm bells triggered by trauma or EMDR to rewire neural circuits damaged by traumas.
However, a simple association between trauma and a psychological outcome is not causally informative. For instance, the umbrella meta-analysis on trauma and mental disorders included 104 studies that assessed trauma retrospectively and only two that used a prospective assessment. None of the studies could rule out potential confounding variables including genetics. In the specific case of borderline personality disorder, the best evidence suggests that childhood trauma is of minimal causal significance. Instead, genetics and unshared environmental factors account for differences in Borderline symptoms.
Some forms of trauma obviously exist and are likely adaptive because they cause painful memories and rumination that motivate a person to avoid the circumstances that led to the traumatizing event (s). But the notion that trauma is a pervasive causal variable, responsible for most psychological suffering is implausible. In the case of borderline personality disorder, the trauma theory is almost certainly wrong. Similar logic likely applies to other cases of mental diseases putatively caused by trauma.
The long shadow of Freud still hangs over psychology and psychiatry. With the help of behavioral genetics and other sophisticated methods of ascertaining causality, we may finally walk out from it.
Ben Winegard is an independent writer and researcher. He holds a Ph.D. in Developmental Psychology from the University of Missouri.
Bo Winegard is the Executive Editor of Aporia.

If you enjoyed this, check out:

Great article!
The reverse causality idea is compelling to me because I have a family member with borderline personality disorder who tried to convince me that I had been abused, both as a child and as an adult. For example she told me that Child Protective Services had been called to check on me as a toddler (not true) and tried to recast a couple of experiences where a boyfriend was just being a bit neglectful as abusive. In another instance, I had a good friend with BPD who hadn't spoken to her father in over a year and consistently told me it was too painful to talk about. Finally, when pressed, she described the incident and it was just her father refusing to pay for her to get her car door fixed. Unsurprisingly, when I told her this didn't seem like a good reason for years of silent treatment, I got silent treatment for a week. Borderline Personality has such a strong impact on the culture, especially leftist culture, and it doesn't get talked about enough.
Nice piece. Your readers may be interested in my, similarly titled, piece, from a month ago: https://triangulation.substack.com/p/the-myth-of-trauma
"The notion of trauma is another powerful tool our culture provides. It gives people meaning but also creates an alibi with the end result of a sense of entitlement."